
SMALLPOX
Smallpox was a highly contagious human disease caused by the virus variolae. There are two strains: variolae major, which had severe symptoms and a very high mortality (20-40%), and variolae minor, which had less severe symptoms and lower mortality (about 1%).
The virus is known to have existed for thousands of years, and has probably killed up to 100 million people in its history, and left 200 million blind and scarred. The disease is at least 3000 years old, confirmed in China and India, with a few isolated cases in North Africa. There is no mention in Europe until the 6th century.
During the 17th and 18th Centuries smallpox was the most serious infectious disease in The West and accounted for a substantial proportion of deaths, especially among town dwellers. The mortality rate varied regionally, with 10% in Europe and 90% in America. Hispanola (modern Haiti and the Dominican Republic) were the first American sites of European contact. Exposure to smallpox during early Spanish attempts to convert the Native populations to plantation slavery exterminated all 3.5 million Native inhabitants of the region.
Smallpox is a poxvirus, characterized by a brick-shape, containing linear double stranded DNA, a disk-shaped core within a double membrane, and a lipoprotein envelope.
The virion contains a DNA-dependant RNA polymerase. This enzyme is required because the virus replicates in the cytoplasm and does not have access to the host's cellular RNA polymerase, which is located in the nucleus.
Smallpox has a single, stable, serotype, which is the key to the success of the vaccine. If the antigenicity varied as it does in influenza, eradication would have failed.
Penetration is usually through the respiratory tract and local lymph nodes and then the virus enters the blood (primary viremia). Internal organs are infected; then the virus reenters the blood (secondary viremia) and spreads to the skin. These events occur during the incubation period, when the patient is still well. The rash is the result of virus replication in the skin, but there may be an immune component as well. Immunity following smallpox disease is permanent; immunity after smallpox vaccination lasts up to ten years.
A person infected with smallpox and overtly sick usually transmits the virus face-to-face in a closed dwelling. There is no infectious subclinical state (no submerged iceberg). Smallpox is characterized in its classical form by the sudden onset of fever, headache, backache, vomiting, marked prostration and even delirium. At this early stage the patient may be very ill and compelled to take to his bed. Early in the illness there may appear in about 10% of patients a fleeting rash in the form of a reddening of the skin, not unlike the rash of German Measles. This is the so-called prodromal rash and, in the absence of a history of exposure to a source of infection, there is nothing about this rash to arouse suspicion of smallpox. The incubation period from exposure to the onset of this feverish illness is nearly always 12 days with very little variation either way.
About two to three days after the onset of illness the true smallpox rash appears. At this time any prodromal rash will be fading. This true or so-called focal rash is normally diagnostic of smallpox and is characteristic both in its evolution and distribution on the body. It begins as tiny discrete pink spots, macules, which enlarge and become slightly raised papules. Each of these progresses by the third day to become a tense blister, 6mm in diameter, deep in the skin.

After two more days the fluid inside becomes turbid and the lesions are not described as pustules but by the older term of pocks. In the following days these shrink and dry up to become hard lentil-like crusts in the skin.

Eventually they separate leaving a sunken scar.

The hard material, which comes away contains smallpox virus in its substance.
The distribution of this focal rash is characteristic, affecting the head and extremities much more than the trunk.
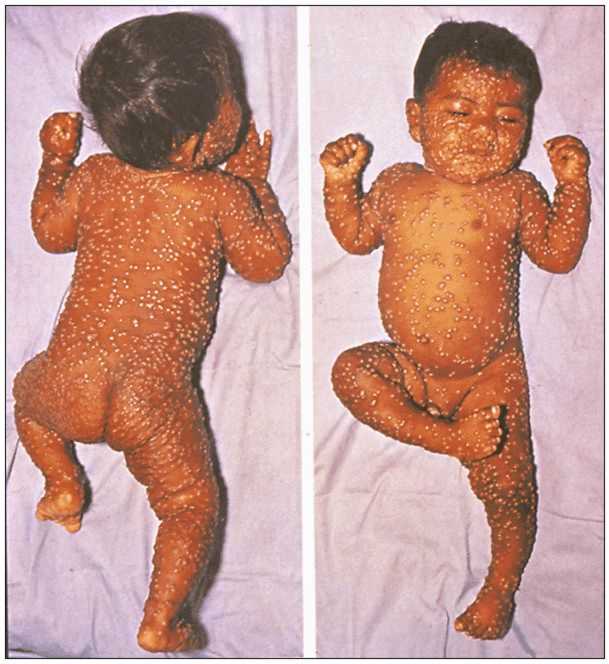
There is some correlation between severity of illness and extent of focal rash. Toxemia (due to massive tissue damage) may be so sever as to cause death even before the rash is fully developed, but more commonly death, if it occurs, will be between the 11th and 15th day of the rash. In severe cases the rash may cover the entire body and the individual lesions run into one another to become confluent.

This patient dies of toxemia soon after this picture was taken.
In 1967 the World Health Organization (WHO) embarked on a World Eradication Program. In the prior year, 10-15 million people had died of smallpox.
Smallpox was a good candidate for eradication because:
1. smallpox virus had a single, stable, serotype
2. there was no animal reservoir and humans were the only hosts
3. the antibody response was prompt, so that exposed persons could be protected
4. the disease was easily recognized clinically, so that exposed persons could be immunized promptly
5. there was no carrier state or subclinical infection
The last recorded natural case was in Somalia in 1977,

but laboratory exposure has caused several small epidemics since. Canada and the US discontinued the practice of vaccination in 1973. The WHO declared the disease eradicated in 1980. Today, only those with immunity due to surviving smallpox disease are protected.